Introduction
SARS-CoV-1 is the SARS virus, which caused the SARS outbreak of 2002.
SARS-CoV-2 is the Coronavirus.
COVID-19 is the disease caused by the Coronavirus, SARS-CoV-2.
COVID-19 stands for “COronaVIrus Disease 2019”.
* Viral infection is the process by which a virus infects a cell and hijacks that cell’s machinery to replicate, i.e. make copies of itself. This is how viruses spread within the body, and it is one of the ways that a virus harms the body.
* ACE2 is a normal enzyme receptor on the surface of many cells in the human body, including the lungs and intestines.
* A protease is an enzyme which can read the sequence of amino acids in a protein and cut up the protein into smaller pieces. The Coronavirus produces two non-functional proteins (pp1a and pp1b), and then uses two proteases to cut up those proteins into smaller functional proteins — which then begin their work of making copies (replicating) of the virus.
* A polymerase is an enzyme which can manipulate DNA, or in this case RNA. The Coronavirus uses polymerases to manipulate its RNA during the process of viral replication, inside an infected cell, and to copy its RNA to make proteins.
* Virulence factors are certain Coronavirus proteins which interfere with the human immune system and help the virus escape from immune system attacks [1].
* Inhibitors are compounds, whether prescription drugs [3] or natural substances [1, 2], which bind to components of a virus to interfere with viral infection and replication. Inhibition of a virus is not a cure; at best, it can make the viral infection less severe.
How the Coronavirus does its damage
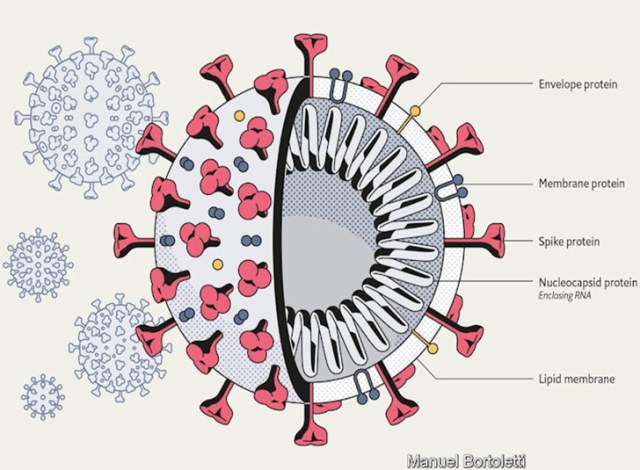
The Coronavirus (SARS-CoV-2) has a spherical shape, like a soccer ball. Inside the sphere is the viruses genes, in the form of RNA. Coronaviruses have no DNA. The RNA is wrapped by a protein nucleocapsid, which serves to protect the RNA, and which will later assist in the viral infection of the host cells.
Other viruses have a protein shell, which your immune system can recognize and attack with antibodies. SARS-CoV-2 has a “host-derived cell membrane”. It makes its shell out of the cell wall from the human cells it infects. So the virus infecting you has part of your cells incorporated into each virus particle.
The spherical membrane around the Coronavirus has hundreds of Spike proteins sticking out on all sides. These Spikes are what allow the virus to infect cells in the human body (host cells).
The Spike is a complex protein; actually, it is three copies of the same protein intertwined. And it looks less like a spike and more like this:

The drawing of the Spike on the left only shows the protein part of the Spike. The drawing on the right also shows the attached sugar groups (oligosaccharides; a light color in the drawing). These sugars are called glycans. The Spike protein is a glycoprotein (a protein with sugar attached). The glycans reduce the immune response of the human body [4]. They limit the accessibility of potentially neutralizing antibodies to the protein part of the Spike. So the sugar groups fend off the immune system. This works because immune system cells and the antibodies they produce are fairly large. They cannot fit between the sugar groups to get at the inner Spike protein.
This Spike has the correct complementary three-dimensional shape to bind to a protein receptor on the surface of many human body cells: the ACE2 receptor (angiotensin-converting enzyme 2). One part of the Spike attaches to the ACE2 receptor of the host cell in the human body, to dock the virus at the cell. Another part of the Spike initiates the “fusion of the viral and cellular membranes” [5], thereby infecting the cell with its RNA. Inhibiting the Spike protein prevents the Spike from attaching to the ACE2 receptor, and prevents infection of the cell by the virus.
With many Spike proteins attached to many ACE2 receptors, they can no longer function in their usual manner. “The angiotensin-converting enzyme 2 (ACE2) is an important regulator of the renin–angiotensin system.” [6] This system plays a pivotal role lung, heart, cardiovascular, and kidney function [7]. The disruption of the system by the binding of the Coronavirus Spike to so many ACE2 receptors throws the regulation of certain organs, especially the lungs and heart, into disorder, causing grave harm. These ACE2 receptors are found in the lungs, heart, kidney, intestines, and the cells that line the blood vessels [8, 9]. And this is one reason why COVID-19 is so severe It attacks organs outside of the respiratory system. It also attacks the respiratory system in a severe and different manner than a flu virus. And cases of Coronavirus often include intestinal symptoms, like diarrhea, due to viral infection of intestinal cells .
Now when the Coronavirus infects a cell in the human body, its viral RNA is treated by the cell like its own RNA. The cell then makes the proteins encoded by the viral RNA. The Coronavirus has three sets of proteins coded into its RNA: polypeptide 1a (ORF1a), polypeptide 1b (ORF1b), and a third set of structural and accessory genes.

Polypeptide 1a and polypeptide 1b (pp1a and pp1b) are long proteins that do pretty much nothing — until two sections of the protein break away and act as proteases: PLpro and 3CLpro. These proteases then cut up the two polypeptides into a total of 16 pieces, including non-structural protein 12 (nsp12), which is RdRp (RNA dependent RNA polymerase), and nsp13, which is Helicase. Both of those proteins are polymerases, which are necessary for the virus to copy and manipulate RNA while replicating. Once the two proteins are cut up into 16 pieces, those proteins, along with the structural and accessory proteins coded by the third section of the viral RNA, can begin making more Coronaviruses to further infect the body. And once the RdRp protein has been made, it can make more proteins from the viral RNA with less reliance on the cellular machinery of the host cell. This allows the virus to replicate more quickly than otherwise.
As new viral components are manufactured within an infected cell, each new virus particle buds off from the host cell. The cell wall bulges outward, with viral RNA and proteins within it. And then it pinches off, forming the new viral particle. This means that the cell membrane around the viral RNA and viral proteins is part of your body’s own cells. It is a piece of a human cell membrane that becomes the viral cell membrane. Other viruses use a protein shell, which can be recognized by the immune system. The Coronavirus uses part of the host’s own cell walls, which cannot be recognized and attacked by the immune system. Then the Spike proteins are coated in sugar groups, protecting that protein from the immune system. In addition, virulence factors also help the Coronavirus evade any attack from the immune system. These factors make the Coronavirus more harmful than viruses such as the flu.
The Spike protein, the proteases PLpro and 3CLpro, the polymerases, RdRp and Helicase, are five targets which researchers have chosen for the inhibition of SARS-CoV-1 or SARS-CoV-2. The inhibitor compounds bind to the target, thereby blocking its function — like when you “forget” to pay your parking tickets, and the city puts a “boot” on your car, thereby “inhibiting” its function. Since these components are essential to viral infection and replication, inhibiting anyone of them is detrimental to the virus and helpful to the patient. Though inhibitors cannot reach every viral particle or viral component, they can slow the virus down, lessening the severity of the disease.
This approach of using inhibitors against viral diseases is not mere theory. It is used in practice against HIV/AIDS and Hepatitis C. HIV is treated with two protease inhibitors [10]. And then Hepatitis C is treated with two proteases and two polymerases [11]. And drugs currently being trialed against SARS-CoV-2 (COVID-19) are believed to work as inhibitors, including the drugs hydroxychloroquine and azithromycin.
Viral inhibitors are the main hope for treatment of COVID-19. Studies are underway, and new research is being published almost every day. Hope is on the horizon.
Ronald L. Conte Jr.
— ENDNOTES —
[1] Wu C, Liu Y, Yang Y, Zhang P, Zhong W, Wang Y, Wang Q, Xu Y, Li M, Li X,
Zheng M, Chen L, Li H, “Analysis of therapeutic targets for SARS-CoV-2 and discovery of potential drugs by computational methods”, Acta Pharmaceutica Sinica B.
https://doi.org/10.1016/j.apsb.2020.02.008
[2] ul Qamar, Muhammad Tahir, et al. “Structural Basis of SARS-CoV-2 3CLpro and Anti-COVID-19 Drug Discovery from Medicinal Plants.” (2020).
https://www.preprints.org/manuscript/202002.0193/download/final_file
[3] Lin, Shen, Runnan Shen, and Xushun Guo. “Molecular Modeling Evaluation of the Binding Abilities of Ritonavir and Lopinavir to Wuhan Pneumonia Coronavirus Proteases.” bioRxiv (2020).
https://www.biorxiv.org/content/10.1101/2020.01.31.929695v2.full
[4] Xiong, Xiaoli, et al. “Glycan shield and fusion activation of a deltacoronavirus spike glycoprotein fine-tuned for enteric infections.” Journal of virology 92.4 (2018): e01628-17.
Click to access e01628-17.full.pdf
[5] Walls, Alexandra C., et al. “Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein.” Cell (2020).
https://www.sciencedirect.com/science/article/pii/S0092867420302622
[6] Prabakaran, Ponraj, Xiaodong Xiao, and Dimiter S. Dimitrov. “A model of the ACE2 structure and function as a SARS-CoV receptor.” Biochemical and biophysical research communications 314.1 (2004): 235-241.
https://www.sciencedirect.com/science/article/pii/S0006291X03026792
[7] Science Direct, “Renin Angiotensin Aldosterone System”, from Encyclopedia of Biomedical Engineering, 2019.
https://www.sciencedirect.com/topics/biochemistry-genetics-and-molecular-biology/renin-angiotensin-aldosterone-system
[8] Zhang, Haibo, et al. “Angiotensin-converting enzyme 2 (ACE2) as a SARS-CoV-2 receptor: molecular mechanisms and potential therapeutic target.” Intensive Care Medicine (2020): 1-5.
https://link.springer.com/article/10.1007/s00134-020-05985-9
[9] Feng, Zhijie, Yan Wang, and Wei Qi. “The Small Intestine, an Underestimated Site of SARS-CoV-2 Infection: From Red Queen Effect to Probiotics.” (2020).
https://www.preprints.org/manuscript/202003.0161/v1
[10] Ghosh, Arun K., Heather L. Osswald, and Gary Prato. “Recent Progress in the Development of HIV-1 Protease Inhibitors for the Treatment of HIV/AIDS.” Journal of medicinal chemistry 59.11 (2016): 5172-5208.
https://pubs.acs.org/doi/abs/10.1021/acs.jmedchem.5b01697
[11] Zając, Marianna, et al. “Hepatitis C-New drugs and treatment prospects.” European journal of medicinal chemistry 165 (2019): 225-249.
https://www.sciencedirect.com/science/article/abs/pii/S0223523419300352